ARTICLES
The Fortune 500 CEOs with the Best (and Worst) Headshots

What do the headshots of the world's top executives have to do with the performance of the companies they lead?
-

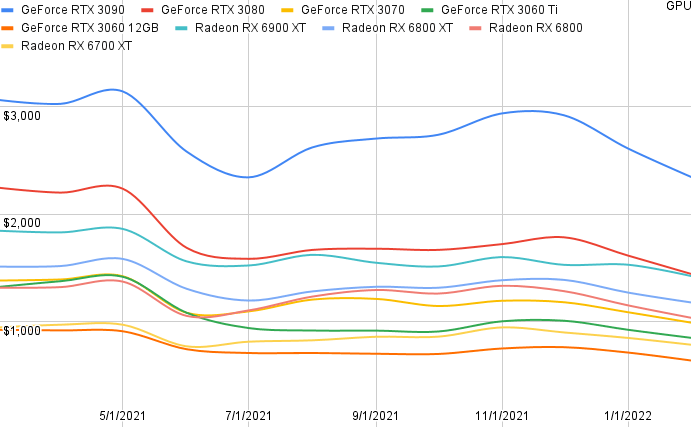
In 2018 I set up a mining rig with dual Radeon RX 470 GPUs. I was frustrated with how much they cost. The 470 was expensive and outdated.
-

Did you order your new iPhone already? If it hasn’t yet arrived, you may be in for a long wait.
-

Zoom towns with high wildfire risk are also seeing the fastest growth in home prices, and therefore the fastest increase in wildfire exposure
-

Discover what our survey of Seniorly users revealed about gender and aging in America in the early months of 2021: a gender gap in stress and connectedness.
-

What do the headshots of the world's top executives have to do with the performance of the companies they lead?
-

The vast majority of people who get payday loans are employed. Here's where they work.
-
Analyzing online reviews of nursing homes to reveal the areas of the countries with the best and worst.
-

As the pandemic unfolded, we used a lot more plastic in 2020 around the world. Will it continue?
-
Home prices spike as people seek out backyards and more space during the pandemic.
-
Analyzing the reasons why people get payday loans.
-

Ranking the Cities with the Most New Homes Built in High-Risk Wildfire Zones
-

Is cannabis cheaper through delivery or at dispensaries during COVID-19?
-

You might graduate with a lot of a debt and very low income, depending on the college.
-

Black neighborhoods pay 20% more in renters insurance.
-

How much of a house's purchase price will the typical annual salary cover in cities across America.
-
Bootcamp graduates are generally pretty satisfied (unless they end up unemployed or in non-technical roles afterwards).
-

In this article, we’ll look at job applications. Are people looking for work currently or still shying away from employment due to the virus?
-

According to our estimate 10.9% of coronavirus cases in the United States are healthcare workers.
-
Just how much do low-income Americans who get pay payday loans pay for housing?
-
Quantifying the devastating impact of COVID-19 on the hourly job market.
-
The places in America with the most and least people above the age of 65 years old.
-
Much of the media hype around blockchain has simmered, but the enterprise is still interested.
-

The states and cities in America with the best and worst rated hospitals according to Medicare data.
-
Higher speeds, lower latency, massive device proliferation, and customized networks. Here's what's coming with 5G.
-
An analysis of traffic death by state, drunk driving, and who buckles their seatbelt.